

Type 1 diabetes is a chronic medical condition that occurs when the pancreas, an organ in the abdomen, produces very little or no insulin. Insulin is an important hormone without which the body cannot utilize glucose for energy. The unutilized glucose circulates in the blood and leads, over time, to serious complications involving the heart, kidneys, eyes, and feet. These patients are also at risk for acute complications such as diabetic ketoacidosis (which may lead to coma), and low blood sugars (hypoglycaemia) that can occur following treatment.
Type 1 diabetes usually begins in childhood or young adulthood, but can develop at any age. The number of people with Type 1 diabetes is on the rise, doubling almost every decade. Type 1 diabetes requires regular blood sugar monitoring and treatment with insulin. Insulin is vital for the survival of people with Type 1 diabetes. Treatment, lifestyle adjustments, and self-care can control blood sugar levels and minimize the risk of disease-related complications.
Depending on their age and level of maturity, children/adolescents should be encouraged to take care of themselves. Diabetes education is mandatory in the management of type 1 diabetes in children/ adolescents
There are unique challenges in caring for children and adolescents with diabetes that differentiate pediatric from adult care. These include the obvious differences in body size, developmental issues such as the unpredictability of a toddler’s dietary intake and activity level, and medical issues such as the increased risk of low sugars (hypoglycaemia) and diabetic ketoacidosis that are distinctly different between adults and children. The risks of diabetic complications are also likely influenced by puberty. Thus, the management of diabetes in children and adolescents with Type 1 diabetes must take into account the age and developmental maturity of the child.
Diabetes is stressful for both the child as well as his/ her family. Diabetes management in children and adolescents becomes more effective when the entire family gets involved. Parents should be alert for signs of depression, eating disorders, or an unexplained loss of weight and seek appropriate medical help. Families should be encouraged to share their concerns with physicians, nutritionists, diabetes educators, psychologists, and other healthcare providers to get help in the day-to-day management of diabetes.
Depending on their age and level of maturity, children/adolescents with Type 1 diabetes should be encouraged to take care of themselves. Very young children cannot be expected to take care of themselves without adult supervision. Even middle school and high school students cannot be expected to independently provide all of their own diabetes management care. This emphasizes the need for parental involvement throughout childhood and adolescence to ensure appropriate self-management and metabolic control. Thus, the education about how to care for a child and adolescent with diabetes must be provided to the entire family unit, emphasizing age and developmentally appropriate self-care and integrating this into the child’s diabetes management. The goal should be a gradual transition toward independence in management through middle school and high school. Adult supervision is vital throughout the transition.
Educating the child with diabetes and his/her about healthy eating habits, exercise, and dosage management of insulin is the most important part of the initial management of the disease. For the preschooler, education should be directed toward the parents and primary caregivers, whereas for most adolescents (after consideration of their emotional and cognitive development), education should be directed primarily toward the patient, with the active involvement of the parents.
Infants & Toddlers (<3 years of age)
Infants and toddlers present unique challenges for the treatment of Type 1 diabetes. The tremendous responsibility of care and fear of hypoglycemia are extremely stressful for families as infants do not exhibit the classic symptoms of hypoglycaemia and are unable to communicate symptoms associated with hypoglycemia. Thus the risk of severe hypoglycemia, with seizures or coma, is highest in this age group. Among toddlers, hypoglycemia is a constant fear, especially when the child refuses to eat. Thus, parents of infants/toddlers need the support of a diabetes team that understands the difficulties of dealing with them and is able to provide emotional support to manage their concerns.
Preschoolers (3–6 years)
Most children in this age-group can participate in their self-management by testing blood glucose, helping to keep records, and in some cases counting carbohydrates. For this group, parents provide care for preschoolers, but others, such as child care providers may also be involved in the care. Undetected hypoglycemia remains a concern because of the variations in activity and food intake characteristic of this age-group, and because of continuing concerns regarding the adverse effects of hypoglycemia on brain development and function.
School-aged children (7–11 years)
In this age group, immediately following diagnosis, children report mild depression and anxiety. This is because children may feel that they are different from their peers due to their diabetes. These usually resolve by 6 months after diagnosis. However, after the first 1–2 years, depressive symptoms increase, and anxiety decreases for boys but increases for girls over the first 6 years after diagnosis. Children with diabetes can take care of their daily diabetes management tasks, such as insulin injections and blood glucose testing with supervision and support from caring and knowledgeable parents. It is important to encourage school-aged children to attend school regularly and to participate in school activities and sports to facilitate the development of normal peer relationships.
Both children and parents fear hypoglycemia and the potential for hypoglycemia to interfere with learning. Most school-age children can recognize symptoms of hypoglycemia and if they are over 12 years old they may be able to take insulin injections of correct dosage by themselves. Children can also be involved in planning their own diet chart.
Adolescents
Adolescence is a period of rapid biological change accompanied by increasing physical, cognitive, and emotional maturity. Many of the diabetes-related activities can interfere with the adolescent’s drive for independence and peer acceptance. Adolescents can perform the tasks of diabetes management, however, they still need help with decision-making about insulin adjustments. Thus, continuing to involve parents appropriately, with shared management, is associated with improved control. During the later adolescent years, the parents and the diabetes care team need to assist them to transition to more independent self-management and to adult diabetes care providers.
Glycemic goals
Glycemic goals should be individualized and lower goals may be reasonable based on benefit-risk assessment.
Plasma blood glucose and HbA1C goals for type 1 diabetes by age group
Self-monitoring of blood glucose (SMBG) using glucose meters has been shown to be associated with improved glycemic control. The frequency of blood glucose monitoring should be adapted to the insulin regimen, the age of the child, and the stability of diabetes. For children with type 1 diabetes, four or more tests per day are generally necessary. Children whose HbA1c is rising or is persistently elevated should have all aspects of their diabetes management reassessed.
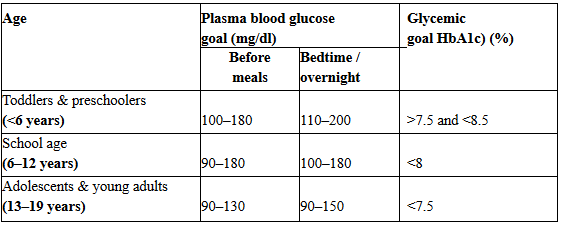
SOURCE: American Diabetes Association
- Blood glucose goals should be higher than those listed above in children with frequent hypoglycemia or hypoglycemia unawareness
- Postprandial blood glucose values should be measured when there is a disparity between pre-prandial blood glucose values and A1C levels



6 thoughts on “Care of Children and Adolescents with Type 1 Diabetes”
After my Diabetes diagnosis. I was constantly dehydrated, I was placed on metformin but worsened over time. My doctor introduced me to Herbal HealthPoint and their successful Diabetes treatment, I immediately started on the herbal treatment. The Diabetes treatment reversed my Diabetes and i lost alot of weights too. Go to ww w. herbalhealthpoint. c om. I am diabetes free